Übersetzt aus dem Englischen:
Erlernen Sie die chirurgische Technik zur Fixation eines Schlüsselbeinbruchs mit der Synthes Superior Schlüsselbeinplatte mit Schritt-für-Schritt-Anleitungen auf OrthOracle. Unsere E-Learning-Plattform enthält hochauflösende Bilder und eine zertifizierte CME des chirurgischen Verfahrens zur Fixation eines Schlüsselbeinbruchs mit der Synthes Superior Schlüsselbeinplatte.
Schlüsselbeinfrakturen sind häufig und machen etwa 2,6% aller Frakturen aus, wobei Frakturen im mittleren Drittel 80% ausmachen. 2-6% treten im medialen Drittel auf, während die verbleibenden 12-16% am lateralen Ende des Schlüsselbeins auftreten. Diese Frakturen kommen am häufigsten bei einer jungen und aktiven Bevölkerung vor.
Die Behandlung solcher Verletzungen kann umstritten sein, da dislozierte mittlere Drittel-Schlüsselbeinfrakturen historisch konservativ mit niedrigen gemeldeten Nicht-Verheilungsraten behandelt wurden. In der Literatur werden jedoch zunehmend deutlich höhere Raten von bis zu 20% berichtet. Es ist allgemein anerkannt, dass diese durch chirurgische Eingriffe erheblich reduziert werden können.
Obwohl bei jedem chirurgischen Eingriff ein gewisses Risiko besteht, zeigen veröffentlichte Ergebnisse auch, dass die Fixation mit Platten und Schrauben sicher durchgeführt werden kann, um ein gutes Ergebnis mit verbesserter Patientenzufriedenheit und einer Reduzierung der Nicht-Verheilungsrate im Vergleich zu konservativ behandelten Frakturen zu erzielen.
Original Intro:
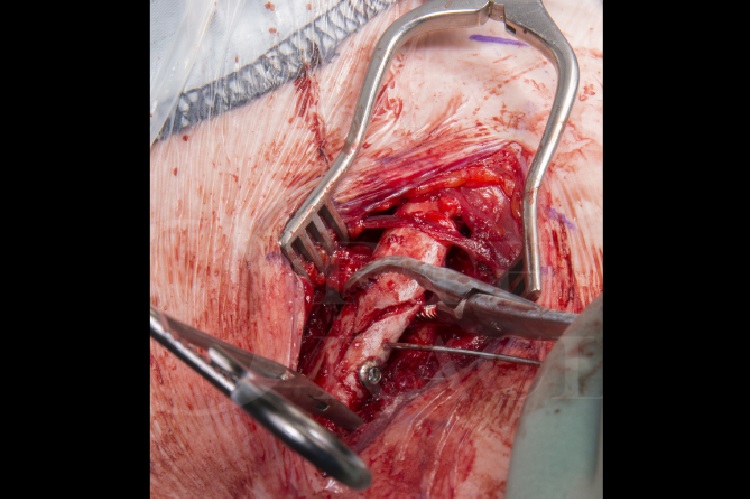
Clavicle fracture: Fixation using Synthes superior clavicle plate
Learn the Clavicle fracture: Fixation using Synthes superior clavicle plate surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Clavicle fracture: Fixation using Synthes superior clavicle plate surgical procedure.
Clavicle fractures are common accounting for around 2.6% of all fractures, with middle third fractures accounting for 80%. 2-6% occur in the medial third, while the remaining 12-16% occur in the lateral end of the clavicle. These fractures most commonly occur in a young and active population.
The management of such injuries can be controversial as historically, displaced mid-shaft clavicle fractures have been managed conservatively with low reported non-union rates. However, more literature has reported much higher rates, up to 20% on occasion. It is widely accepted that this can be reduced significantly with surgical intervention.
Whilst there is some risk with any surgical intervention, the published results also demonstrate that plate and screw fixation can be performed safely to give a good outcome with improved patient satisfaction and a reduction in the non-union rate compared to conservatively managed fractures.
For displaced lateral end clavicle fractures, there is a higher rate of non-union and therefore, the threshold for surgical fixation is lower. Options for surgical fixation include specific lateral end anatomic clavicle plates utilising a variety of locking screw options for the smaller lateral fragment. Some plates allow reconstruction of the ruptured coracoclavicular ligaments with a non-absorbable material to augment and support the repair. If standard internal fixation is not possible due to comminution, these fractures can also be managed with a hook plate. The lateral end of this plate hooks under the acromion and butresses the lateral clavicle from displacing superiorly. The disadvantage with this type of fixation is that it needs to be removed once the fracture has healed to avoid impinging on the rotator cuff and causing a cuff tear. Whilst in situ, it may also physically limit the arc of movement in the shoulder.
There are many implant companies with clavicle specific plates. My preference is for the Synthes LCP clavicular (Locking Compression Plates). These are anatomically contoured and sided plates with either a superior or supero-anterior plates option for mid-shaft clavicle fractures. Superior clavicle plates tend to require less contouring. Theoretically, the medial screws are also directed further away from the neuro-vascular bundle. The plates and screws on the Synthes set are made of stainless steel with the “combi-hole” design allowing the option of either locking or non-locking screws within the same hole. The Synthes clavicle set also provides useful instruments to facilitate the surgical exposure and fracture reduction.
Author: Mr Sam Chan, FRCS (Tr & Orth).
Institution: The Queen Elizabeth hospital, Birmingham, UK.